
#12 TWO SEMINAL PEER-REVIEWED STUDIES
- Aug 23, 2023
- 11 min read
Updated: Sep 2, 2023

The following studies use the pain fiber F-NCS, the initial EDx now used in the Neural-EDx™ F-EMG The F-NCS, without the potentiometer objective recording, was at that time termed V-sNCT.
Study #1
https://ispub.com/IJPSP/2/2/6139 Predicting Nerve Root Pathology With Voltage-actuated Sensory Nerve Conduction Threshold
INTERNET SCIENTIFIC PUBLICATIONS
Original Article
R Cork, S Saleemi, L Hernandez, T Schult, S Brandt
Keywords
Citation
R Cork, S Saleemi, L Hernandez, T Schult, S Brandt. Predicting Nerve Root Pathology With
Abstract
Voltage-actuated sensory nerve conduction threshold (V-sNCT) is a quantitative test of sensory function. This study compares the sensitivity, specificity, and predictive value of V-sNCT to physical examination for the presence of nerve-root adhesions visible on epidurogram. Predicted abnormal nerve roots by V-sNCT and/or physical examination were compared with abnormal nerve roots documented by abnormal epidurogram in forty-nine patients with L5/S1 radicular back pain. Sensitivity, specificity, and predictive value for V-sNCT predicting nerve root pathology were 94.6%, 70.2%, and 91.0%, respectively, compared to 61.7%, 72.3%, and 87.6%, respectively, for prediction by physical examination alone. In addition, area under ROC Curve and relative risk for V-sNCT were significantly more predictive of nerve-root pathology than physical examination (p<0.05). Prediction of abnormal nerve-root pathology with spf-NCS is superior to prediction from neurological examination.
Introduction
Sensory neurological examination is an important part of any physical examination. This part of the physical examination takes on even more importance in the workup of the patient with chronic pain. During World War II, Dr. George Riddoch, a neurologist in the British Army, developed a logical approach to the sensory examination with the concept of identifying “signature” surface areas highly correlated with specific anatomic dermatomes, which, in turn, are associated with specific nerve roots.1 Later, the concept of current perception threshold (CPT) was developed to quantitate level of sensory deficit.2 Problems developed with this diagnostic technique, however, with significant variability associated with changing skin resistance.3 Recently, the concept of voltage-actuated sensory nerve conduction has resulted in the development of a new instrument to quantitate sensory function. This instrument provides testing which is voltage mediated, and results are independent of changes in skin resistance. The purpose of this study was to assess how well V-sNCT worked in predicting nerve root pathology as defined by filling defects on epidurogram prior to epidural lysis of adhesions.
Methods
After IRB approval and informed consent, patients with L5 or S1 radicular back pain scheduled for lysis of epidural adhesions4 were studied. All patients underwent pre-procedure testing. All patients received catheter-directed lysis of adhesions, during which an epidurogram was done with 10 ml of Omnipaque-180 contrast. Predicted abnormal nerve roots identified by prior to the procedure were compared with abnormal nerve roots documented by abnormal epidurography of the nerve root. In addition, neurological examinations were conducted relating to the nerve roots tested. Neurological examination for L5 and S1 nerve roots were conducted as described by Hoppenfeld.5 Neurological exam associated with L5 and S1 consisted of a motor, reflex (except for L5), and sensory test. Motor test for L5 was to test dorsiflexion of the big toe with the extensor hallucis longus. The examiner supported the patient's foot with one hand around the calcaneus and then placed his/her thumb in such a position that the patient must dorsifex his/her great toe to reach it. The examiner opposed the dorsiflexion by placing his/her thumb on the nail bed of the great toe and fingers on the ball of the foot. Motor test for S1 was to test plantar flexion and eversion of the foot by opposing this motion with pressure on the head of the fifth metatarsal. There is no reflex to test for L5 function, but S1 was tested with the Achilles tendon reflex. Sensation for L5 was tested on the dorsum of the foot; sensation for S1 was tested at the lateral malleolus. In addition to the L5 and S1 nerve roots, major peripheral nerves tested included the superior and inferior gluteal nerves, as well as the sciatic, tibial and common peroneal nerves.
The statistical analysis tested the predictive power of V-sNCT compared to the predictive power of physical examination, using the abnormal epidurogram as the pathological standard. Analysis was with chi-square and ROC analysis, 6 with significance defined at p<0.05. Sensitivity, specificity, and predictive value for V-sNCT and physical findings as predictors of root pathology were calculated using the following formulas: 6
Confidence intervals of the areas under the ROC curves were used to test for significant difference between prediction with V-sNCT and neurological examination at p<0.05. Also, relative risk and 95% confidence intervals were calculated for abnormal epidurogram, given an abnormal V-sNCT or an abnormal neurological examination at L5 and S1. Visual analog scores (VAS) were compared using Student's paired t-test. Significance was p<0.05.
Results
Forty-nine patients were studied, 28 males and 21 females. Age (mean±SEM) was 49±2, weight 86±3 kg, height 172±1 cm. Twenty-five patients had undergone previous back surgery; all had a diagnosis of lumbar radiculitis. VAS pain scores prior to procedure were 8.6±0.2 and one month after the procedure VAS pain scores were 4.4±0.4 (p<0.05). V-sNCT test results and epidurograms for a patient with an S1 lesion are shown in Figure 1 and Figure 2. Sensitivity, specificity, and predictive value for V-sNCT predicting nerve root pathology were 94.6%, 70.2%, and 91.0%, respectively, and an ROC curve was calculated (see Figure 3). Area under the ROC curve is 0.82 0.04 (p<0.001; 95% CI 0.76-0.90) for V-sNCT, compared to 0.67 0.04; 95% CI 0.60-0.74) for neurological examination (p<0.05).
Figure 1 – 2
V-sNCT and epidurogram prior to lysis of adhesions at S1. Note hypoesthesia of right S1 on the V-sNCT graph (1) correlates with lack of filling of the right S1 nerve root on epidurogram (2). Left is left and right is right on epidurogram.
Figure 1-2




Figure 3 – 4
V-sNCT and epidurogram after lysis of adhesions at S1. Note that V-sNCT (3) has returned to normal and right S1 nerve root (4) now fills with contrast.




Receiver Operating Characteristic (ROC) curves comparing the effectiveness of V-sNCT pain fiber NCS and neurological examination in predicting nerve root pathology. Better predictors are indicated with movement of the reference line to the upper left.
Results for all nerve roots tested are displayed in Figure 4 for V-sNCT and Figure 5 for the neurological examination. Sensitivity, specificity, and predictive value were 61.7%, 72.3%, and 87.6%, respectively, for prediction of abnormal epidurogram by physical examination alone.
Finally, relative risk (with 95% confidence interval) of abnormal epidurogram, given an abnormal spf-NCS is 4.67 (2.50-8.69), compared to 1.40 (1.17-1.66) given an abnormal neurological examination. These data are summarized in the following table 1:

Figure 8

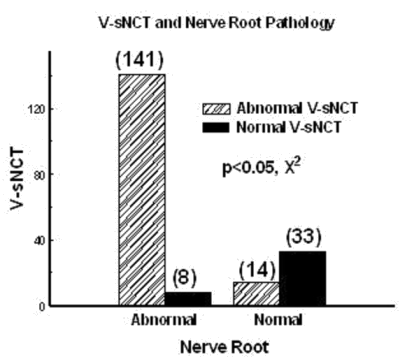


Figure 9
Prediction of nerve root pathology by neurological examination. Abnormal and normal nerve roots can be predicted by neurological examination (p
p<0.05, compared to Neurological Examination.

Discussion
Voltage-actuated sensory nerve conduction threshold is a direct quantitative sensory test which provides a reproducible functional assessment of the peripheral sensory nervous system by measuring that voltage intensity which initiates membrane potential changes to propagate nerve impulses. This study used a V-sNCT device. A predecessor, the Neurometer assesses sensory function by measuring current output, which varies with changes in skin resistance. Although sensitivity with V-sNCT was superior to neurological examination, specificity was no different than the neurological examination. However, both the V-sNCT and neurological examination give the clinician the ability to test various branches of the peripheral nerves, which may result in further definition of the location of entrapment/pathology to specific nerve segments.
Conclusion
The purpose of this study was to compare the sensitivity and specificity of V-sNCT for the presence of nerve-root adhesions visible on epidurogram. Voltage-actuated sensory nerve conduction threshold provides the pain-management specialist with a sensitive and specific tool for prediction of nerve root pathology. Advantages of V-sNCT includes simplicity, decreased test time, small intra-patient variability, and decreased sensitivity to changes in skin resistance. It is a better predictive test than the neurological examination because it is a more sensitive test. In addition, because the patient is blinded to the V-sNCT results, it may be a very good test for detecting malingering. This study demonstrates that prediction of nerve-root pathology with V-sNCT is superior to prediction of nerve-root pathology from neurological exam alone.
References
1. Walton J, Gilliatt RW, Hutchinson M, McArdle MJF, O'Brien MD, Thomas PK, Willison RG. Aids to the examination of the peripheral nervous system. London: WB Saunders; 1986.
Chado HN. The current perception threshold evaluation of sensory nerve function in pain management. Pain Digest 1995; 5:127-134.
American Association of Electrodiagnostic Medicine. Technology review: The Neurometer current perception threshold (CPT). Muscle and Nerve 1999; 22:523-531.
Lou L, Racz G, Heavner J. Percutaneous epidural neuroplasty. In Waldman S, editor. Interventional Pain Management, 2nd ed. Philadelphia. WB Saunders; 2001. p 434-45.
Hoppenfeld S. Physical examination of the spine and extremities. Norwalk (CT): Appleton & Lange; 1976. p. 252-3.
Browner WS, Newman TB, Cummings SR. Designing a new study: Diagnostic tests. In Hulley SB, Cummings SR, editors. Designing Clinical Research. Baltimore: Williams and Wilkens, 1988. p. 87-97.
{full-citation}
Note: At several conferences Dr. Cork has stated that A-delta F-NCS is the real gold standard by which other methods should be compared, because it a functional assessment. Abnormal anatomy does not prove pathology (abnormal function).
Study #2
Multicenter Study - January 2010 – Sponsored by the AASEM
Paradoxical Relationship: A-Delta Function and VAS
Authors: Randall Cork, MD, PhD, Michael Bezel, MD
Abstract:
The A-delta pain fiber nerve conduction study is a functional NCS (F-NCS) that measures the sensitivity of these fast pain fibers, which are known to down-regulate soon after injury. This study compares changes in the sensitivity of the A-delta fibers in pathological nerve-roots with changes in the patient’s subjective visual analog score (VAS). A significantly close relationship was found between the change in voltage required to cause an action potential (nerve impulse) in the A-delta fibers of the pathological nerve-root and changes in the subjective VAS rating. The findings support the utility of the A-delta F-NCS for detecting the level and side of painful radiculopathy and measuring changes in pain.
Introduction:
An objective marker associated with the patient’s subjective pain perception has been an elusive challenge. A multitude of scales have been proposed in the attempt to quantify the severity of pain experienced by the patient and to quantify the response to treatment. The visual analog scale (VAS) has been widely used as a gauge of pain severity in acute and chronic pain. ,,,
The F-NCS is used to locate pain generators. For several decades physiology texts have described that during the first Epicritic Phase of sensory nerve injury the A-delta fibers up-regulate causing a withdrawal reflex. This is shortly followed by the Protopathic Phase in which Guyton & Hall Textbook of Medical Physiology explains that the poor localizing C-Type fibers begin to up-regulate. Concerning this Protopathic Phase Guyton states; “It explains why so many patients have serious difficulty localizing the source of some types of chronic pain. ” Cork, et al showed that the nerve-root adhesion causing radicular pain is associated with hypo-sensitivity of A-delta fibers in the associated peripheral nerve. Other studies have used hypo-sensitivity of the A-delta fibers as detected by the F-NCS as an objective marker for pain. ,,
The purpose of this study was to survey the clinical association between the patient’s VAS pain rating and sensitivity of the A-delta fibers as measured by the F-NCS.
Methods: A study group was formed from members of the American Association of Sensory Electrodiagnostic Medicine certified in A-delta F-NCS electrodiagnostic examination (EDx). After IRB approval of the study by AASEM the study group members were asked to submit A-delta F-NCS studies for those patients who reported a change in VAS after treatment for pain and comparative F-NCS was performed. After one month, 83 pairs of VAS ratings and the associated graphs of the A-delta F-NCS made on the same day were received. Data analyzed included the pre-treatment and post-treatment VAS pain scores, difference in the voltage required to cause an action potential of the A-delta fibers in the pathological nerve-root identified by the pre A-delta F-NCS of the peripheral nerve associated with the nerve-root identified by the pre A-delta F-NCS, sex and spinal region (cervical or lumbar). Data were analyzed using repeated-measures analysis of variance. Results were considered significant if p<0. 05.
Results: Change in VAS and voltage inducing an action potential are shown in Figure 1. Both VAS and voltage decreased with treatment (p<0. 001).

Both sex and spinal level were significantly associated with threshold level (p<0. 05), but neither was significantly associated with VAS. A-Delta threshold voltage decreased from 28. 4±1. 4 v (SEM) (n=43) to 18. 7±1. 4 v for males (p<0. 001) and from 24. 6±1. 1 (n=40) to 16. 5±1. 0 v for females (p<0. 001). Figure 2 illustrates the different voltage thresholds for each sex and how threshold level changed with treatment for males and females.

Threshold voltage for cervical dermatomes was significantly lower than threshold voltage for lumbar dermatomes (p<0.05). Threshold voltage decreased from 23.0±1.4 v (n = 36) to 14.6 ± 1.0 v (p<0.001) for cervical dermatomes and from 29.3±1. 1 v (n = 47) to 20 ± 1.0 v (p<0.001) for lumbar dermatomes. Figure 3 illustrates how lumbar voltage thresholds were significantly higher than cervical voltage thresholds (p<0.05) and how both lumbar and cervical thresholds decreased with treatment (p<0.001).

In contrast to threshold voltage, VAS response was not different for males compared to females or for cervical dermatomes compared to lumbar dermatomes. Figure 4 shows the response to treatment for both males and females. Although there is a significant treatment effect (p<0.001), there is no difference in VAS response based on sex.


Figure 5 shows a similar response to treatment for both the cervical and lumbar region. Again, although there is a significant treatment effect (p<0.001), there is no difference between cervical and lumbar VAS responses.
Figure 5. Change in VAS for both cervical and lumbar regions in response to treatment. Although there is a significant treatment effect (p<0.001), there is no difference in treatment response based on spinal region or level.
Discussion: These data represent the results of a survey of members of the American Association of Sensory Electrodiagnostic Medicine. Thus, the responses to treatment reported may be biased by members submitting “typical” responses that make the treatment look good. Nonetheless, the focus of the survey was not on the effectiveness of treatment, but on how the response to treatment, as measured by VAS, was associated with the response to treatment as measured by the threshold voltage of the A-delta fibers. On the basis of these results, A-delta fiber threshold voltage is a good independent marker of pain decrease with successful treatment, independent of the pain report given by the patient. This is a significant finding, as patient perceptions are very subjective and affected by many extraneous variables, including malingering.
Why females should have lower A-delta threshold voltages is an interesting question that certainly deserves more research. Similarly, why the cervical region would have lower A-delta fiber voltage thresholds than lumbar region is another potential area of investigation. However, the study data shows clearly that A-delta function as measured by voltage threshold is dependent of both sex and spinal region. With adjustments for sex and spinal region, A-delta hypo-sensitivy appears to be an objective marker for measuring the success of therapeutic interventions.
Conclusions:
A-delta sensitivity/function as measured by voltage threshold using the F-NCS is related to the patient’s pain perception. As A-delta sensitivity improves from hyposensitivity to normal sensitivity, pain decreases; as A-delta sensitivity/function deteriorates, pain increases. Females have lower A-delta fiber voltage thresholds than males, and the cervical region exhibits lower A-delta fiber voltage thresholds than the lumbar region, but the A-delta voltage thresholds drop independently of sex and spinal level with treatment. In contrast, the VAS responses are not different based on either sex or spinal level, but VAS drops significantly in concert with the drop in A-delta fiber sensitivity/function. In general, A-delta sensitivity/function measured by A-delta small pain fiber nerve conduction study F-NCS is an excellent objective measure of pain change following treatment, and a practical and painless electrodiagnostic procedure for detecting the side and level of painful radiculopathic pain generators.
References
Bijur PE, Silver W, Gallagher EJ: Reliability of the visual analog scale for measurement of acute pain. Academy of Emergency Medicine. 2001 Dec;8(12):1153-7.
Bijur PE, Latimer CT, Gallagher EJ: Validation of a verbally administered numerical rating scale of acute pain for use in the emergency department. Academy of Emergency Medicine. 2003 Apr; 10(4):390-2.
Holdgate A, Asha S, Craig J, Thompson J: Comparison of a verbal numeric rating scale with the visual analogue scale for the measurement of acute pain. Emergency Medicine (Fremantle). 2003 Oct-Dec;15(5-6):441-6.
Salaffi F, Stancati A, Silvestri CA, Ciapetti A, Grassi W: Minimal clinically important changes in chronic musculoskeletal pain intensity measured on a numerical rating scale. European Journal of Pain. 2004 Aug;8(4):283-91.
Guyton & Hall Textbook of Medical Physiology 11th Ed. , 2006: 601
Cork RC, Saleemi S, Hernandez L, Schult T, Brandt S: Predicting nerve root pathology with voltage-actuated sensory nerve conduction threshold. The Internet Journal of Anesthesiology, (6:1), 2002.
Badruddoja M, Bush IM, Irshad M, Bush AP, Aguillar F: Chronic prostatitis causing pelvic pain due to sacral entrapment. Presented at the American College of Surgeons, October 10, 2008.
Hernandez L, Chaubey R, Cork RC, Brandt S, Alexander L: Treatment of Piriformis Syndrome with Botox. The Internet Journal of Anesthesiology, www. ispub. com, 6(2), 2003.
Raza H, Zavisca F, Hernandez L, Brandt S, Chaubey R, Isaac I, Cork R, Alexander J, Alexander L: Treatment of Piriformis Syndrome with Botulinum Toxin-A, Using V-sNCT to Aid Diagnosis. The Internet Journal of Anesthesiology,www. ispub. com, 7(1), 2003.
